
Erysipelas in birds is usually an acute overwhelming and fatal infection. It is most commonly seen in turkey flocks but is now being seen more in free range layer flocks. It is also the cause of swine erysipelas (diamond disease), joint ill in lambs or post dipping lameness in sheep. In addition to mortality it is associated with lack of finish in meat birds and infertility in male breeding birds with drops in egg production of layers. It is a zoonosis causing local or sometimes septicaemic infections. It is seen most commonly in fish handlers, butchers, veterinary surgeons and farmers.
Table of Contents
Synonyms
None in birds but known as erysipeloid in man and diamond disease in pigs.
Cause
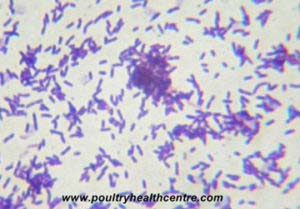
Erysipelothrix rhusiopathiae, a gram positive slender, slightly curved, non-motile rod. It can be easily decolourised with Grams stain and thus appear to be gram negative. It may form filaments. Pin point colonies can be seen on blood agar after 24 – 48 hours and alpha zones of haemolysis appear later. Three types of colony have been described; smooth, rough or intermediate. It is a facultative anaerobe. Serotypes 1, 2 and 5 of the 26 serovars are most commonly isolated.
Host
Juvenile to adults, turkeys, fowl and gamebirds, ducks and geese, doves and pigeons (experimental infection), pigs, sheep, cattle, fish, dolphins and crocodiles.
Transmission
The source of infection may not be obvious. Sources can include contact with pigs, sheep, rodents, infected carcases, contaminated fish meal and land that has had infected animals on it. It has been shown to survive but not grow in soil for at least 35 days. Infection is more common on earth floored houses than concrete ones. Infection is believed to occur through damaged mucous membranes or skin cuts and artificial insemination. Oral infection is the most likely route and less likely is infection through cuts in the skin. Mechanical transmission of infection is assoicated with biting flies such as mosquitos, stable and horse flies. A small number of birds can become inapparent carriers. Outbreaks are often associated with cold wet weather.
Clinical signs
Presents in two forms – acute and endocarditis. Observations: If not found dead, fevered, ruffled feathers, anorexia and lethargy may be seen. Head and neck: no specific signs. Musculoskeletal: no specific signs. Thorax and abdomen: diarrhoea. Egg abnormalities: there may be a drop in egg production. Endocarditis may be associated with cachexia, weakness, anaemia and death,
Pathology
DiagnosisPetechial haemorrhages on the heart, abdominal fat, congestion and enlarged friable liver, spleen and kidney, sticky mucus in intestinal tract and a generalised septicaemia (bloody discolouration of the abdominal contents). In lame birds a white fibrinopurulent pus can be found in the joints. Those with endocarditis have yellow vegetative nodules in the heart.
The history, post mortem lesions and isolation or demonstration of E.rhusiopathiae will confirm the diagnosis. Bacterial isolation is more successful from dead then moribund birds. Samples sites should include liver, spleen, bone marrow and heart blood. Bacteria will be seen in impression smears from the liver.
Differential diagnoses
Fowl cholera, peracute Newcastle disease, avian influenza, acute colibacillosis and salmonellosis.
Treatment
Antibiotic therapy can help e.g. Amoxycillin. Vaccination including using autogenous vaccines can be successful. There is a wide variation in the response to both treatment and vaccination. Relapse after treatment is common. A combination of vaccination and treatment has proved to be beneficial.
Prevention
In the UK a dead injectable vaccine is available to immunise turkey flocks. All housing should be thoroughly cleaned and disinfected prior to restocking. Erysipelas is a particularly resistant organism. A 2% solution of sodium hydroxide has been found to be effective whilst phenols and related disinfectants are less effective. Ensure that all disinfectants are used at the most concentrated levels recommended.
Erysipelas is the 8th commonest diagnosis made by my local AHVLA labs. Details of species affected, clinical signs and post mortem lesions observed can be found by clicking here.